Analyzing the Shortcomings in Smart Healthcare for Remote Home Care: A Case Study of the Taiwan Market
Zhang Lee and Chen Yang
Department of Medical Science, Sun Yat-Sen University, Guangzhou, China
Published Date: 2024-07-11DOI10.36648/2471-9781.10.1.392
Zhang Lee* and Chen Yang
Department of Medical Science, Sun Yat-Sen University, Guangzhou, China
- *Corresponding Author:
- Zhang Lee
Department of Medical Science, Sun Yat-Sen University, Guangzhou,
China,
Email: leezang@yahoo.com
Received date: June 10, 2024, Manuscript No. IPJHMM-24-19153; Editor assigned date: June 13, 2024, PreQC No. IPJHMM-24-19153 (PQ); Reviewed date: June 27, 2024, QC No. IPJHMM-24-19153; Revised date: July 04, 2024, Manuscript No. IPJHMM-24-19153 (R); Published date: July 11, 2024, DOI: 10.36648/2471-9781.10.1.392
Citation: Lee Z, Yang C (2024) Analyzing the Shortcomings in Smart Healthcare for Remote Home Care: A Case Study of the Taiwan Market. J Hosp Med Manage Vol.10 No.1:392.
Abstract
In Taiwan, remote healthcare was initially limited to telemedicine services, and the systematic development of remote care was relatively delayed. It was not until 2007 that the Department of Health of the executive Yuan first initiated the 'Remote Care Pilot Program,' followed by the 'Remote Care Service Improvement and Quality Enhancement Plan' in the subsequent year. In 2010, Taiwan officially launched the 'Remote Health Care Services Development Plan' and established a dedicated project office, marking the comprehensive start-up of remote care services. This stage saw significant contributions from artificial intelligence aids and ICT remote transmission technologies, greatly promoting the application of smart healthcare in home care. This study aims to explore the strategic gaps in the application of smart healthcare in home remote care. By analyzing gaps in 'legal regulations,' 'economic factors,' 'user behavior habits,' 'policy and culture,' and 'environment and technology,' this study employs a mixed-methods approach. Particularly, it uses the Analytic Hierarchy Process (AHP) to construct a weighted ranking of these strategic gaps. Through in-depth interviews with doctors and smart healthcare experts and the collection of 16 valid AHP questionnaire samples, which cover both industry and academia with a balanced distribution, the survey results are ensured to be representative and reliable. The findings indicate that 'legal regulations' are considered the most critical strategic gap that needs to be addressed first, followed by 'user behavior habits.' This suggests that when designing smart healthcare applications, greater consideration needs to be given to user acceptance and habits. By systematically analyzing and addressing these strategic gaps, this study not only provides solutions to issues in the application of smart healthcare in home remote care but also offers valuable references for future research and practice, aiming to make home remote care services more comprehensive and efficient.
Keywords
Smart healthcare; Telemedicine; Home remote care; Analytic Hierarchy Process (AHP); Expert in-depth interviews
Introduction
The year 2020 marked the beginning of commercial 5G deployment in Taiwan. Characterized by its high speed, high reliability and low latency, 5G technology is regarded as a key driver for the integration of network platforms and the healthcare industry. As pointed out by Jingjing et al., [1], these characteristics of 5G are instrumental in mitigating the deficiencies and imbalances in Taiwan's healthcare resources development, especially considering the aging population issue that Taiwan is facing. The urgency for the application of smart healthcare becomes particularly evident. Furthermore, Yi et al., [2] suggest that the advantages of 5G's high speed, low latency, and high capacity should be fully utilized to facilitate the integration of 5G networks with smart mobile healthcare services, which will effectively address the core issues currently faced by the healthcare industry. As the technology industry continues to progress and Taiwan's population structure becomes increasingly aged, the traditional healthcare industry is no longer sufficient to meet the modern demands for medical services. As stated by Liwen et al., [3], in response to this trend, traditional face-to-face medical services must shift towards telemedicine models. To address the long-term care needs of the elderly and the medical requirements of patients with chronic diseases, the healthcare industry is widely adopting information and communication technologies to enhance the convenience of home-based remote care. This transformation indicates that Taiwan's future health care services industry will broadly adopt new modes of service. As the issue of aging intensifies, the increasing proportion of the elderly population makes elderly care a significant topic in contemporary society. Many geriatric diseases progress rapidly and require urgent treatment within a short window of time. Delays in detection and intervention can severely hinder timely treatment opportunities. Therefore, the early detection and prompt management of health issues are crucial for the well-being of the elderly. Against this backdrop, utilizing high-tech means such as 5G to achieve real-time monitoring of the health status of the elderly and to provide timely feedback to medical institutions has become an effective strategy to safeguard the health of the elderly. Additionally, early detection of diseases and timely treatment not only effectively reduce medical costs but also help alleviate the pressure on government healthcare expenditures. Given the mobility challenges faced by the elderly, the application of smart healthcare technologies significantly lowers their difficulties in accessing medical resources. The low latency of 5G technology plays a vital role in ensuring the timeliness of medical data transmission and the success rate of diagnosis and treatment. Moreover, by analyzing monitoring data and establishing health models to predict future health conditions, the mortality rate from age-related diseases can be effectively reduced, thereby extending the expected lifespan of society. The home care model not only saves on manpower costs by enabling a few caregivers to efficiently manage many elderly individuals, but it also reduces the economic and time costs associated with travel. Additionally, this model helps alleviate the issue of uneven distribution of medical resources across regions, particularly in sparsely populated or economically underdeveloped areas, thereby better addressing the care challenges faced by the elderly. However, the application of smart healthcare technology also faces numerous challenges and issues. First are legal issues; remote healthcare cannot obtain comprehensive information as face-to face consultations do, presenting potential risks that could lead to misdiagnosis or insufficient care. Therefore, laws need to further clarify the scope of practice and responsibility distribution in telemedicine. Secondly, economic factors must also be considered, such as defining whether the costs of care products are borne by individuals or paid by the government, and how to balance the costs of services. Lastly, the security and privacy of personal data are equally important, and there must be legal provisions to ensure the safety of these data. These issues are key to the research discussed herein, aiming to propose solutions to promote the development and application of smart healthcare technology.
Materials and Methods
Definition and trends of smart healthcare
Smart healthcare is defined by Jie et al., [4] as the trend of integrating advanced technologies such as the Internet of Things (IoT), cloud computing and high-level analytics into existing medical processes. The application of these technologies in the field of smart healthcare is extensive, having propelled the market entry of remote healthcare, remote patient monitoring, integrated electronic medical record management systems, patient wearable devices, online medical consultations and appointments and AI-assisted diagnostics. In this context, the prospects for the application of 5G in smart healthcare are shown to be exceptionally vast. The concept of "Smart Earth" was first introduced in 2009 and since then, its significance has gradually been recognized globally, leading to the emergence of a series of related concepts, including "smart healthcare." With the rapid development of information technology, the integration of IT and traditional medical practices has accelerated and is now comprehensively applied within Taiwan's healthcare services. The deep integration of information technology has significantly propelled the innovation of Taiwan's medical system, enhancing both medical service models and personal health management.
At the governmental level, smart healthcare provides more scientific decision support, primarily reflected in the following aspects: Firstly, the deep mining and analysis of patient medical data based on big data systems; secondly, smart healthcare technologies significantly enhance the timeliness of rational decision-making by health-related departments in Taiwan; and thirdly, the ability to establish smart emergency systems that maintain contact with large hospitals or small clinics, achieving timely and effective monitoring and management.
For businesses, smart healthcare brings substantial benefits to the development of telemedicine platforms and medical device apps. Patients can interact in real-time with data on medical information platforms through home apps or self-diagnosis platforms, providing convenient services to patients and significantly reducing the worry for their family members about needing to travel.
With continuous innovation in telemedicine technology internationally, the focus of smart healthcare technology development is shifting towards the research and development of AI-based early screening tools. Early screening gathers extensive data and with the help of AI, assists doctors in diagnostics. This not only effectively reduces the time doctors spend reviewing cases but also alleviates the screening burden on healthcare professionals and enhances diagnostic accuracy, aiding doctors in making better medical decisions. This contributes to the early detection and treatment of diseases, reducing the waste of health insurance resources on the care of chronic diseases.
In the future, the application of smart healthcare in home remote care will become more widespread, with a sharp increase in the demand for home IoT health terminals, and the interoperability of medical information will become more comprehensive [5]. This indicates the potential of smart healthcare technologies and their pivotal role in the future medical field.
Categories of remote care
Remote care is defined as the use of 5G communication network technologies and software to transmit health and medical information for patients in need of urgent treatment across different locations and to support communication and learning among medical teams from various countries globally, thereby enhancing the quality of remote medical care services and extending them to home life support [6]. Currently, Taiwan's remote care market can be categorized into three main types:
• Combining 5G and AI technologies for remote medical diagnoses and even surgeries, with cases already implemented internationally. Especially after the COVID-19 pandemic in 2020, the development of remote care has accelerated significantly, driving progress in the service system. Given Taiwan's shortage of medical personnel, rising medical costs, increasing chronic disease population and the impact of the pandemic, it is foreseeable that future care trends will evolve towards remote, non-contact applications.
• A significant increase in community day care centers and care points, effectively promoting elderly community participation.In community smart nursing clinics, the public can use exercise equipment, measure blood pressure, etc., with related records subsequently uploaded to a cloud platform and integrated with medical imaging systems, connecting to the outpatient system of health posts, allowing physicians to monitor the physiological health data of the public in real time during the diagnostic process, thereby encouraging residents to form healthy living habits.
• Home remote care, specifically targeting elderly individuals living alone. Considering that many elderly people's children are unable to stay nearby due to work, the placement of smart medical devices becomes particularly important to prevent emergencies from going unnoticed, leading to emergency medical situations.
These innovative remote care models not only bring revolutionary changes to Taiwan's healthcare service system but also pave new paths for global health management. The ongoing development in this field is expected to greatly enhance the efficiency andq uality of medical services, especially in addressing the global aging challenge.
Home remote care
Pei-Yu et al., [7] pointed out that home remote care is an essential component of the long-term care system, encompassing a variety of professional services, greatly facilitating the various issues faced by patients receiving care at home [8]. Specifically, long-term care services mainly include the following aspects:
Care services: Divided into home services, day care, and family hosting.
Respite services: Including home respite and institutional respite.
Home nursing: Provided by professional home nurses, including visiting patients' homes for guidance and treatment.
Rehabilitation services: Rehabilitation tasks performed by therapists at patients' homes.
Assistive device support: Involving the purchase, rental, and improvement of barrier-free home environments.
As Taiwan’s aging population continues to grow, the demand for long-term care is increasing. Therefore, developing Tele- Home Care (THC) has become a significant direction in smart healthcare. The primary advantage of THC is that it enhances the capabilities of family caregivers and improves the quality of life for the entire family. For those care recipients who do not require daily medical assistance, THC facilitates convenient twoway interaction with professional medical personnel through wired or wireless transmission and equipped micro physiological parameter sensors. This not only reduces the travel burden for both parties but also enhances the mobility and disease selfmanagement of the care recipients.
This study focuses on the categories of home remote care, exploring the use of smart electronic medical devices and 5G communication technologies to enable elderly patients or their relatives to monitor health indicators such as blood pressure and blood sugar at home and store data in real-time on device apps, further uploading it to the smart hospital center service platform. This process not only allows medical personnel to conduct timely remote disease detection and tracking but also greatly facilitates home patients, eliminating their need to visit hospitals or clinics.
The shortcomings in smart healthcare for remote home care
Laws and regulations: Taiwan's regulations in the field of telemedicine were relatively strict until the outbreak of the COVID-19 pandemic, which saw them become more lenient. Similar to Japan's approach of easing regulations through administrative interpretation, Taiwan also adjusted its "Regulations on Telemedicine," but unlike Japan's comprehensive opening strategy, Taiwan only expanded the scope of application, mainly targeting groups under home quarantine or isolation. Additionally, prior to 2018, Taiwan's "Physician Act" stipulated that, except in remote areas, medical services in other areas required the physical presence of a physician. However, from January 10, 2018, the Ministry of Health and Welfare introduced the "Draft Regulations on Telemedicine," further broadening the scope of telemedicine. This included "follow-up treatment within three months after discharge for acute inpatients," "residents of residential long-term care facilities," among other new applicable groups, significantly expanding the target audience for telemedicine services.
The rapid development of electronic technology and the rise of the ICT industry have facilitated the widespread use of technologies such as 5G, video transmission, bluetooth, and wireless networks, providing technical support for real-time home remote care and treatment. However, according to the current "Physician Act," telemedicine has not been fully opened to all Taiwanese people and is still awaiting further policy adjustments.
Legal responsibilities associated with telemedicine are also complex. Remote physicians may only provide professional opinions without establishing a substantial physician-patient relationship, which is referred to as "remote consultation" rather than "telemedicine." Once a physician-patient relationship is established, the lack of face-to-face examination, such as palpation or potential distortions in image transmission, introduces uncertainty into the determination of negligence liability. This uncertainty may become a psychological barrier for physicians resistant to opening telemedicine.
Moreover, when significantly opening telemedicine, other detailed issues need consideration, such as ensuring that medical actions are performed to apply for health insurance payments, which might require recording the entire process to prove informed consent. Additionally, if physicians prescribe medications, patients might still need to physically visit pharmacies to collect their prescriptions, which is not a complete solution for those with mobility issues. Thus, how to reasonably open online pharmacies and address the opposition from physical pharmacies is also a critical issue that needs to be resolved in telemedicine policies. The implementation of these measures will have a profound impact on the development direction and industry trends of telemedicine services in Taiwan.
Economic factors: Due to the intensifying trend of an aging population [9] and the chronic nature of diseases resulting from advances in medical technology, along with changes in family structures and a reduction in family caregiving functions, elderly individuals face significant difficulties accessing medical care due to reduced mobility or disability. This situation leads to a significant increase in medical costs for the elderly. At the same time, Wenyi et al., [10] have noted that remote areas face severe issues with the uneven distribution of medical resources. In this context, the intervention of remote care becomes particularly necessary, but the high costs of remote care are not affordable for every family, especially as the level of service increases, which also raises the costs. Therefore, economic factors become a critical consideration for many families when choosing remote care services.
One of the primary issues facing remote care is the network connectivity of smart healthcare devices. Although 2020 marked the commercial debut year of 5G technology, there are still issues with unstable connections or interruptions under the 4G network environment. Additionally, each home smart healthcare device operates on its independent system, lacking necessary integration. While technological devices are advanced and visually appealing, their high costs and solutions that do not target core pain points limit their widespread adoption. Although 5G networks offer the possibility of real-time data transmission, their high communication costs also deter many families with limited financial resources.
If the remote care industry could nurture several teams with an ecosystem mindset to collaboratively create an interconnected working model, a new care paradigm could potentially emerge. This model would redefine the framework of remote care through technology and innovation, likely playing a significant role in enhancing care quality, reducing costs and more broadly disseminating smart healthcare devices.
Policy and culture: In 2021, the head of Taiwan's Central Health Insurance Administration under the Ministry of Health and Welfare announced that the year would be designated as the inaugural year for telemedicine health insurance payments, with an allocation of 100 million New Taiwan Dollars to include telemedicine within the scope of health insurance coverage. Initially, this policy will cover ENT (Ear, Nose, and Throat), dermatology, emergency, and outpatient services in 50 townships and districts. In the emergency sector, the subsidy per patient varies from a minimum of 507 New Taiwan Dollars to a maximum of 2340 New Taiwan Dollars depending on the triage category; for outpatient teleconsultations, a uniform subsidy of 500 New Taiwan Dollars is provided. Additionally, in 2021, the Health Insurance Administration evaluated the data flow and administrative processes of telemedicine and explored the possibility of integrating home services, long-term care, and telemedicine.
However, currently only certain departments have opened up to the use of telemedicine, and not all types of diseases can receive medical services remotely. The future development of telemedicine within the health insurance system remains unclear, and whether it will be fully opened is still uncertain [11].
In the digital health care industry, the widespread adoption of mobile devices and IoT medical equipment has become an irreversible trend. However, these devices pose data security risks during the information collection and transmission processes. For example, data may be corrupted during transmission, tampered with by humans, or hacked via Bluetooth capabilities, all of which can pose serious threats to patients receiving remote care. Consequently, the U.S. Food and Drug Administration (FDA) has issued guidelines requiring IoTenabled medical devices to have adequate data security protections. Despite this, the rapid development of mobile device technologies, primarily smartphone apps, and their short market lifecycle mean that manufacturers aiming to quickly bring products to market may not fully consider data security and privacy protection. Since 2015, Taiwan's Ministry of Economic Affairs has implemented a voluntary security certification mechanism for apps, but further mandatory implementation could hinder this rapidly changing industry. Therefore, further development at the policy level is still needed.
From a cultural perspective, Taiwan society typically discourages leaving the elderly or patients alone at home, as any malfunction in remote care systems could pose a direct threat to their safety. This cultural characteristic adds significant sociopsychological barriers that must be overcome for the implementation of remote medical services. Therefore, future policy-making and technological innovations must take these cultural factors into account to ensure the widespread acceptance and effective implementation of remote medical services.
Additionally, users are highly concerned about the privacy protection of their personal data. While real-time access to medical health information facilitates medical decision-making, it is also susceptible to hacker attacks. According to monitoring by the Ministry of Health and Welfare, Taiwan's government medical information system can experience up to tens of thousands of cyberattacks each night. For example, Under Armour's health application was hacked in February 2018, resulting in the leakage of approximately 150 million user records. In 2013, a hospital in Los Angeles was hacked and had to pay a significant amount of Bitcoin to ransom encrypted electronic medical records. In 2017, 47GB of medical data stored in an Amazon S3 Repository by a company was illegally accessed.
In the context of the digitalization of medical information, non-medical Information and Communication Technology (ICT) companies may gain access to personal medical and health data. The HITECH Act, passed in the United States in 2009, established clear privacy and security regulations for collaborations between non-medical and medical institutions. However, devices such as Apple watch smartwatches and fitness trackers, as well as data transmission on cloud platforms, may collect substantial amounts of users' physiological data without needing to cooperate with medical institutions, creating legal loopholes.
Medical devices are generally categorized into three or four risk levels for market review. Most health and medical apps are primarily used to record physiological information, but some apps claim to convert smartphones into medical devices such as stethoscopes or combine with external devices for diagnosis or treatment. If the operation of these apps involves medical professionals, safety concerns are minimal; however, if they are entirely operated by users, errors in devices that periodically record physiological information could lead to diagnostic errors.
Currently, post-market monitoring of these technological products mainly relies on product liability and consumer protection laws, with administrative regulations rarely requiring apps to collect and process safety information after market entry. The regulation becomes more challenging with apps developed by foreign companies. Strengthening continuous monitoring and improvement of these products post-market is a significant challenge in future policymaking and in changing user behavior.
Environment and technology: The development of smart healthcare, while full of potential, also faces significant challenges [12]. Firstly, it encounters issues related to standardization, accuracy, and the acquisition, storage, and processing of big data. Key questions include: Who has the right to benefit from this data? Which medical teams or top medical experts are needed to review this data? Moreover, the development of medical artificial intelligence relies on vast amounts of medical data, often facing high costs and poor data quality.
The development of smart healthcare information systems requires close collaboration between medical and technical professionals. However, these two types of professionals differ in their characteristics: the former excels in patient communication, while the latter communicates with machines. In most cases, achieving deep communication between the two is challenging, yet their effective collaboration is essential for indepth research and application of the technology.
Secondly, the high degree of specialization in healthcare and information technology, coupled with information asymmetry and the lack of a common language for deep communication, presents another challenge. While technology is crucial, it should not dominate the healthcare industry. Ignoring this point can lead to project failure.
The third challenge is discussing smart healthcare without the support of a reliable medical team. For example, there are over 500 "diabetes management platforms" available on the App store, but very few are widely used by medical teams and patients. Even wearable devices, despite being purchased, have few continuous users. Without professional support and ongoing improvements from medical teams, these devices are easily abandoned by users.
Finally, the lack of a sustainable business model is a significant challenge. For instance, although telemedicine has played a positive role in improving care quality and preventing patient regret, the monthly fee for Changhua Christian Hospital’s telemedicine service is only 500 New Taiwan Dollars. This model is difficult to sustain. Patients often choose to stop paying for the service after experiencing noticeable short-term improvements, reflecting the issue that high-quality medical services in Taiwan's healthcare system often do not receive corresponding economic returns. Ongoing operational challenges may lead to the discontinuation of many effective medical methods, ultimately harming patient interests.
Reasons for selecting the Taiwan market as a case study
The application of AI technology in the medical field is increasingly widespread, demonstrating significant advantages in diagnostic techniques, and has become a major trend in Taiwan's healthcare market. Traditional Chinese medicine's "observation, listening, questioning and pulse-taking" methods now seem outdated compared to the precision and rigor of modern medical technology. AI has found an ideal application in the medical industry, with Taiwan currently utilizing various types of medical robots, including surgical robots, gastrointestinal inspection and diagnostic robots, rehabilitation robots and other therapeutic robots. For instance, therapeutic robots have been instrumental in improving the quality of life for Alzheimer's patients.
In medical applications, AI not only enhances diagnostic accuracy but also reduces patients' reliance on social services. Especially in handling complex diseases, AI technology can consolidate global case data into a vast database and retrieve critical information within milliseconds. AI systems based on computer vision, deep learning, and neural networks can also achieve early identification and diagnosis of neurological diseases such as Alzheimer's.
In Taiwan, over 85% of individuals aged 65 and above suffer from at least one chronic disease. Chronic diseases, defined as health conditions lasting more than three months, require continuous or long-term management. Remote care technology allows these patients to maintain optimal health, which for elderly patients means extended life expectancy and reduced time and effort spent on managing their conditions and frequent hospital visits. According to the American Association of retired persons, 80% of seniors prefer to receive medical care at home.
According to the United Nations' 2019 World Population Prospects report, the global elderly population is projected to increase by nearly 2 billion over the next 30 years, with the total global population expected to reach 9.7 billion by 2050, approaching the 10 billion mark, and reaching 11 billion by the end of the century. As human life expectancy increases and global birth rates decline, regions with net population reductions are expanding, and the global aging issue is becoming more pronounced. In Taiwan, currently, 1 in every 11 residents is aged 65 or older, a relatively high proportion. It is projected that by 2050, 1 in every 6 people globally will be over 65, with the elderly population accounting for 16% of the total population. The current trend of global population aging has profound implications for the demographic structure of societies and inevitably affects the composition and function of every social family.
Research framework
This study employs expert interviews and the Analytic Hierarchy Process (AHP) as the primary research tools. Firstly, the research theme was determined based on the research background and motivation. Subsequently, relevant literature and information in this field were collected and reviewed. Through in-depth analysis, synthesis, and integration of these materials, the theoretical framework and empirical foundation of the study were established.
On this basis, the first layer of the AHP method was used to extract key strategic sub-factors obtained from expert interviews. These sub-factors serve as the cornerstone for constructing the subsequent research model, providing a scientific basis for questionnaire design. Following this, experts in the field were invited to complete the questionnaires, and the proposed strategies were analyzed in depth to distill effective strategic recommendations.
First layer of the AHP structure
To facilitate the organization of this study, the AHP hierarchy structure includes the goal layer, criterion layer and index layer, as shown in Figure 1. Additionally, this study further defines the five criterion layers as follows:

Figure 1: First layer of the AHP structure.
• Laws and Regulations (A)
• Economic Factors (B)
• Policy and Culture (C)
• User Behavior habits (D)
• Environment and Technology (E)
The corresponding third-level evaluation criteria are defined as A1, B1, C1, D1, E1, and so on.
Expert in-depth interviews
Categories of expert interviews: Expert interviews can be categorized into three types based on their structure: Structured interviews, semi-structured interviews, and unstructured interviews [13]. The definitions and characteristics of these three types of interviews are detailed below:
Structured interviews: In this type of interview, the researcher designs a series of closed-ended questions in advance. During the interview, the researcher asks these predetermined questions one by one, and the interviewee responds based on pre-prepared answers. The main advantage of this method is the ease of recording and analyzing data. However, its limitation lies in the difficulty of obtaining indepth and diverse insights, as the interviewee's responses are often restricted and may not fully reflect their genuine thoughts.
Semi-structured interviews: In this interview mode, the researcher designs a set of guidelines rather than specific closed-ended questions. Within this framework, the interviewee can freely express their views, and the researcher may ask new questions based on the interviewee's responses for deeper exploration. This interview type maintains the focus of the discussion while offering sufficient flexibility, which helps improve the authenticity and validity of the data.
Unstructured interviews: In unstructured interviews, the researcher does not set any closed-ended questions in advance, allowing the interviewee to freely express their true thoughts during the interview. The direction of the interview is guided by the interviewee's immediate ideas and feelings. This interview format is highly beneficial for deeply exploring the interviewee's personal experiences and genuine feelings, but it also requires more time and presents greater challenges in data organization and analysis.
Reasons for choosing semi-structured interviews
Considering the three types of in-depth interviews, this study selects semi-structured interviews as the primary research method [14]. Following the literature review in chapter 2, this study constructs the first layer of the AHP hierarchy to identify potential shortcomings or gaps in the application of smart healthcare in home remote care. Based on this framework, indepth opinion interviews were conducted with scholars and experts in the relevant field.
The reasons for adopting semi-structured interviews are that this method maintains the focus of the research while providing sufficient flexibility, allowing interviewees to demonstrate the depth and breadth of their thinking in their responses. During the interviews, we posed the same questions to different experts, collecting both the differences and commonalities in their answers, and systematically categorizing and organizing the collected information. This approach not only enriches the content of the research but also provides solid data support for further in-depth studies.
Analytic Hierarchy Process (AHP)
Based on the five application gaps identified from the literature review in chapter 2, this study constructs the first layer of the Analytic Hierarchy Process (AHP) framework. To establish this framework and deepen the analysis, we first selected a group of technical experts, professors, and experienced practitioners with a strong background in smart healthcare and remote care for expert interviews. The purpose of these interviews was to gather their insights and evaluations regarding these gaps.
The expert interviews helped to identify the second-level indicators of the AHP framework, significantly enhancing the credibility of the study. Subsequently, using the Analytic Hierarchy Process (AHP), we designed an AHP questionnaire and distributed it to a second group of experts, different from those in the initial interviews. The questionnaire was scored based on specific AHP evaluation scales. Through systematic analysis of the questionnaire data, we calculated the weights of each influencing factor in safety management, thereby objectively revealing the relative importance of each factor in risk management and compiled a comprehensive assessment report [15].
Finally, based on the questionnaire analysis results, we further consulted a third group of experts to discuss the management implications and gap strategy analysis reflected in the data. This process not only deepened the understanding of the application gaps in smart healthcare but also provided scientific basis and strategic guidance for practical implementation (Table 1).
| Scale | Significance | Meaning |
|---|---|---|
| 1 | Be of equal importance | The two elements have the same importance |
| 3 | Slightly important | One of the two elements is more important than the other |
| 5 | Obviously important | One of the two elements is obviously more important than the other |
| 7 | Strongly important | One of the two elements is much more important than the other |
| 9 | Extremely important | One of the two elements is absolutely more important than the other |
| 2, 4, 6, 8 | The compromise between the above two adjacent judgments | Quantitative degree of compromise between the above two adjacent standards |
Table 1: AHP evaluation scale.
AHP execution steps
The execution steps are as mentioned in Figure 2.

Figure 2: Execution steps of AHP.
AHP analytic hierarchy process algorithm
After the establishment of AHP matrix, it is necessary to calculate its vector value for weight. The following four approximate methods were proposed to find the orientation value:
Line vector average standardization method
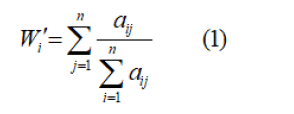
i,j=1,2……,n
Standardized method of column average
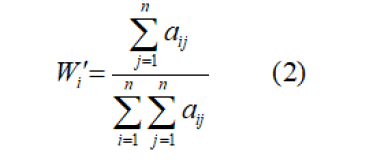
i,j=1,2……,n
Standardization method of row vector sum reciprocal
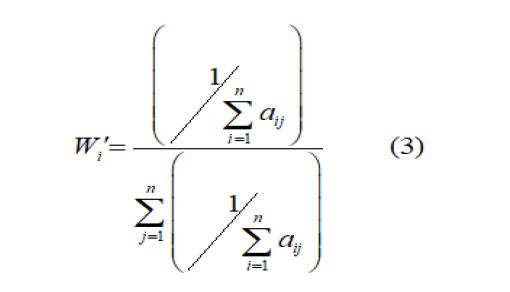
i,j=1,2……,n
Column vector geometric mean standardization method
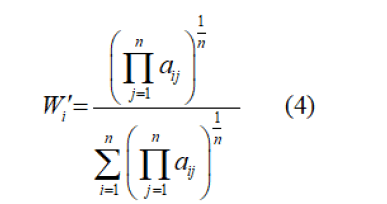
i,j =1,2,.......,n
When calculating the vector value, AHP method uses the first method to calculate the average value of row vectors. Because most of the matrices are inconsistent, the accuracy of this method is better. After calculating the vector, if you want to determine the consistency before and after, you need to calculate the Consistency Index (C.I.) value, and the formula is:
According to the formula, we need to find λ value before calculating C.I.; Therefore, using the weight w obtained above, we first calculate the Consistency vector, which is represented by the ν symbol, so as to obtain the λ value. The formula is as follows:
i,j =1,2,.......,n
After the consistency vector is obtained, the λ value can be obtained by calculating the arithmetic average of its ν value, and the formula is:
Finally, the λ value can be replaced by others to get the C.I. value; C.I.=0 means that the judgment before and after is completely consistent.
When R.I.<0.1, it can be regarded as having better consistency.
According to the research conducted by Dak Ridge National laboratory and Wharton School, the positive and negative matrices generated from evaluation scales 1-9 produce different C.I. values under different levels, which is called Random Index (random index; R.I.) and the ratio of C.I. value to R.I. value is called Consistency Ratio (consistency ratio; C.R.) namely.
Therefore, Chen et al., pointed out that the consistency of the matrix is very high when the value of C.R. is less than 0.1 [16].
Results
AHP second index layer
Based on the second-tier indicators of five application gaps identified in the literature, the first batch of experts was interviewed. After the interviews, unnecessary indicators were deleted, and indicators deemed very important by the experts were added. The final indicators which were considered in the interview has shown in (Table 2).
| Laws and regulations | Irrelevant telemedicine law guarantees the relationship between doctors and patients |
| Liability for medical negligence is not easy to divide | |
| The standard for judging the behaviour of health insurance payment is vague | |
| User behavior habits | Concerns about personal data disclosure |
| The information system APP fails to fully control and ensure information security | |
| Inability to access timely medical quality | |
| Economic factors | Smart medical equipment has a high unit price |
| Requires a high income level | |
| High network communication costs | |
| Policy and culture | Clinics are not fully integrated into medical insurance |
| Information security issues bear the risk of starvation | |
| Conflicts with traditional ideas | |
| The acceptance of smart medical applications among the elderly in biased areas is low | |
| Environment and technology | A sustainable business model is lacking |
| A reliable medical team is lacking | |
| Cooperation between high-end information personnel and medical staff is needed | |
| Acquisition, storage and processing of big data |
Table 2: AHP hierarchical analysis method second layer indicators.
Data compilation of expert questionnaires
Previous research indicated that when comparing two factors, the amount of content involved can influence the judgment of the respondents [17]. Generally, a range of 7 ± 2 is more suitable. We conducted a limitation at 9, and allowed expressing the difference between them on a scale of 1-9. When comparing, it is necessary to make n (n-1)/2 pairwise judgments, providing more information and allowing for a more reasonable ranking through repeated comparisons across various aspects (Table 3).
| Table degree | Meaning |
|---|---|
| 1 | Ci element and Cj element have the same influence |
| 3 | Ci element has a slightly stronger influence than Cj element |
| 5 | Ci element has stronger influence than Cj element |
| 7 | The influence of Ci element is obviously stronger than Cj element |
| 9 | The influence of Ci element is absolutely stronger than Cj element |
| 2,4,6,8 | The ratio of the influence of Ci element to Cj element is between the above two adjacent levels |
| 1,1/2,…,1/9 | The ratio of the influence of Ci element to Cj element is the reciprocal number above |
Table 3: 9-Importance levels and their values.
Table 3 The levels of importance and their respective numerical assignments used in the Analytic Hierarchy Process (AHP) to compare elements.
Random Index (RI) values for matrices of different orders, which are used in AHP to evaluate the consistency of pairwise comparison matrices. The RI values were determined in Table 4.
| Order | 1* | 2* | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
| RI | 0 | 0 | 0.58 | 0.9 | 1.12 | 1.24 | 1.32 | 1.41 | 1.45 |
Table 4: RI Values with matrix order 1-9.
Order 1 and 2 showed RI=0, due to the consistent of the positive reciprocal matrices.
Construction of discriminant matrix and solution of weight
Based on the index system and using the above-mentioned scaling method, a questionnaire survey was conducted using the expert consultation method. The second batch of 16 experts in this smart medical field were selected to independently score the importance of the index. The scoring results were discussed and summarized internally, resulting in the following pairwise discriminant matrix (Table 5).
| Laws and regulations | User behavior habits | Economic factors | Policy and culture | Environment and technology | |
|---|---|---|---|---|---|
| Laws and regulations | 1 | 2 | 3 | 4 | 6 |
| User behavior habits | 0.50 | 1 | 2 | 2 | 3 |
| Economic factors | 0.33 | 0.50 | 1 | 1 | 2 |
| Policy and culture | 0.25 | 0.50 | 1 | 1 | 2 |
| Environment and technology | 0.17 | 0.33 | 0.50 | 0.50 | 1 |
Table 5: Discriminant matrix of AHP index layer.
Maximum characteristic root of the judgment matrix (λmax=5.0166) was calculated by MATLAB software, and average random consistency index (RI=1.12) was determined by Table 4.
In order to check the consistency of the judgment matrix, it is necessary to calculate the Consistency Index (CI) using the following formulation:

Random Consistency Ratio (CR) was calculated by the following formulation:

Therefore, it was concluded that the results of the AHP have satisfactory consistency, indicating that the distribution of weight coefficients was very reasonable. Besides, the weight of index were calculated by MATLAB software (Table 6).
| Index layer | Weight |
|---|---|
| Laws and regulations | 0.4416 |
| User behavior habits | 0.2339 |
| Economic factors | 0.1312 |
| Policy and culture | 0.1239 |
| Environment and technology | 0.0695 |
Table 6: AHP index layer weight.
For each index weight, we used the AHP to determine the index weight of each index layer.
Construct judgment matrix was named as  all CI and CR were calculated by the formulations above.
all CI and CR were calculated by the formulations above.
Firstly, λmax of indicators in laws and regulat ons was 3.0000, and CI was 0 (Table 7). Based on RI=0.58, CR=0 was less than 0.1, it can be considered as a reasonable construct on of the judgment matrix. The weight of the each index layer was calculated and shown in the Table 8.
| Irrelevant telemedicine law guarantees the relationship between doctors and patients | Liability for medical negligence is not easy to divide | The standard for judging the behavior of health insurance payment is vague | |
|---|---|---|---|
| Irrelevant telemedicine law guarantees the relationship between doctors and patients | 1 | 3 | 3 |
| Liability for medical negligence is not easy to divide | 0.33 | 1 | 1 |
| The standard for judging the behavior of health insurance payment is vague | 0.33 | 1 | 1 |
Table 7: Discriminant matrix of indicators of laws and regulations.
| Index layer | Weight |
|---|---|
| Irrelevant telemedicine law guarantees the relationship between doctors and patients | 0.6 |
| Liability for medical negligence is not easy to divide | 0.2 |
| The standard for judging the behavior of health insurance payment is vague | 0.2 |
Table 8: Weight of indicators of laws and regulations.
λmax of indicators in user behavior habits was 3.0000, and CI was 0 (Table 9). Based on RI=0.58, CR=0 was less than 0.1, it can be considered as a reasonable construct on of the judgment matrix. The weight of the each index layer was calculated and shown in the Table 10.
| Concerns about personal data disclosure | The information system APP fails to fully control and ensure information security | Inability to access timely medical quality | |
|---|---|---|---|
| Concerns about personal data disclosure | 1 | 1 | 2 |
| The information system APP fails to fully control and ensure information security | 1 | 1 | 2 |
| Inability to access timely medical quality | 0.50 | 0.50 | 1 |
Table 9: Discriminant matrix of user behavior habits index layer.
| Index layer | Weight |
|---|---|
| Concerns about personal data disclosure | 0.4 |
| The information system APP fails to fully control and ensure information security | 0.4 |
| Inability to access timely medical quality | 0.2 |
Table 10: Weight of user behavior habits indicator layer.
λmax of indicators in user economic factors was 3.0092, and CI was 0.0046 (Table 11). Based on RI=0.58, CR was calculated as 0.0079, which was less than 0.1. Therefore, it was considered that the results of AHP have satisfactory consistency, and the distribution of weight coefficients were very reasonable. The weight of the each index layer was calculated and shown in the Table 12.
| Smart medical equipment has a high unit price | Requires a high income level | High network communication costs | |
|---|---|---|---|
| Smart medical equipment has a high unit price | 1 | 2 | 3 |
| Requires a high income level | 0.5 | 1 | 2 |
| High network communication costs | 0.33 | 0.5 | 1 |
Table 11: Discrimination matrix of economic factors index layer.
| Index layer | Weight |
|---|---|
| Smart medical equipment has a high unit price | 0.5396 |
| Requires a high level of income | 0.297 |
| High network communication costs | 0.1634 |
Table 12: Weight of economic factor indicators.
λmax of indicators in policy and culture was 4.0211, and CI was 0.0070 (Table 13). Based on RI=0.9, CR was calculated as 0.0078, which was less than 0.1. Therefore, it was considered that the results of AHP have satisfactory consistency, and the distribution of weight coefficients were very reasonable. The weight of the each index layer was calculated and shown in the Table 14.
| Clinics are not fully integrated into medical insurance | Risks of capital security problems | Conflicts with traditional ideas | The acceptance of smart medical applications among the elderly in biased areas is low | |
|---|---|---|---|---|
| Clinics are not fully integrated into medical insurance | 1 | 2 | 4 | 5 |
| Risks of capital security problems | 0.5 | 1 | 2 | 3 |
| Conflicts with traditional ideas | 0.25 | 0.5 | 1 | 2 |
| The acceptance of smart medical applications among the elderly in biased areas is low | 0.2 | 0.33 | 0.5 | 1 |
Table 13: Discriminant matrix of policy and culture indicators.
| Index layer | Weight |
|---|---|
| Clinics are not fully integrated into medical insurance | 0.5068 |
| Risks of capital security problems | 0.2641 |
| Conflict with traditional ideas | 0.1428 |
| The acceptance of smart medical applications among the elderly in biased areas is low | 0.0863 |
Table 14: Weight of policy and culture indicators.
λmax of indicators in policy and culture was 4.0042, and CI was 0.00714 (Table 15). Based on RI=0.9, CR was calculated as 0.0015, which was less than 0.1. Therefore, it was considered that the results of AHP have satisfactory consistency, and the distribution of weight coefficients were very reasonable. The weight of the each index layer was calculated and shown in the Table 16.
| A sustainable business model is lacking | A reliable medical team is lacking | Cooperation between high-end information personnel and medical staff is needed | Acquisition, storage and processing of big data | |
|---|---|---|---|---|
| A sustainable business model is lacking | 1 | 2 | 2 | 5 |
| A reliable medical team is lacking | 0.5 | 1 | 1 | 3 |
| Cooperation between high-end information personnel and medical staff is needed | 0.5 | 0.5 | 1 | 3 |
| Acquisition, storage and processing of big data | 0.2 | 0.33 | 0.33 | 1 |
Table 15: Discrimination matrix of environmental and technical indicators.
| Index layer | Weight |
|---|---|
| A sustainable business model is lacking | 0.4488 |
| A reliable medical team is lacking | 0.2346 |
| Cooperation between high-end information personnel and medical staff is needed | 0.2346 |
| Acquisition, storage and processing of big data | 0.0819 |
Table 16: Weight of environmental and technical indicators.
Integrate all the above contents, consistency ratios and weights of AHP criteria layer are presented in the Tables 17 and 18.
| Criterion layer | Evaluation criterion | Consistency Ratio (CR) | Weight/ranking |
|---|---|---|---|
| Laws and regulations (A) | A1~A3 | 0 | 0.4416/1 |
| User behavior habits (D) | D1~D3 | 0 | 0.2339/2 |
| Economic factors (B) | B1~B3 | 0.0079 | 0.1312/3 |
| Policy and culture (C) | C1~C4 | 0.0078 | 0.1239/4 |
| Environment and technology (E) | E1~E4 | 0.0015 | 0.0695/5 |
Table 17: Consistency ratio and weight sorting of AHP criteria layer.
| Primary index | Weight | Secondary index | Weight | Comprehensive |
|---|---|---|---|---|
| Laws and regulations | 0.4416 | Irrelevant telemedicine law guarantees the relationship between doctors and patients | 0.6 | 0.26496 |
| Liability for medical negligence is not easy to divide | 0.2 | 0.08832 | ||
| User behavior habits | 0.2339 | The standard for judging the behavior of health insurance payment is vague | 0.2 | 0.08832 |
| Concerns about personal data disclosure | 0.4 | 0.09356 | ||
| The information system APP fails to fully control and ensure information security | 0.4 | 0.09356 | ||
| Inability to access timely medical quality | 0.2 | 0.04678 | ||
| Economic factors | 0.1312 | Smart medical equipment has a high unit price | 0.5396 | 0.070796 |
| Requires a high level of income | 0.297 | 0.038966 | ||
| Policy and culture | 0.1239 | Clinics are not fully integrated into medical | 0.5068 | 0.062793 |
| Risks of capital security problems | 0.2641 | 0.032722 | ||
| Conflicts with traditional ideas | 0.1428 | 0.017693 | ||
| The acceptance of smart medical applications among the elderly in biased areas is low | 0.0863 | 0.010693 | ||
| Environment and technology | 0.0695 | A sustainable business model is lacking | 0.4488 | 0.031192 |
| A reliable medical team is lacking | 0.2346 | 0.016305 | ||
| Cooperation between high-end information personnel and medical staff is needed | 0.2346 | 0.016305 | ||
| Acquisition, storage and processing of big data | 0.0819 | 0.00569 |
Table 18: AHP index data induction.
Reasons for ranking evaluation criteria
In this study, the AHP questionnaire filled out by the second batch of experts was used to obtain the weight ranking of the application gaps of smart medical care for home remote care. Firstly, the study obtained preliminary results based on the literature survey. Then, the experts were asked why the current weight ranking was formed, which further established the depth and breadth of the study.
Through extensive literature investigation and analysis, this study identified five key application gaps and defined them as the five main criteria layers of AHP. After the first batch of experts reviewed and screened out some unnecessary evaluation indicators, each criterion layer included several evaluation indicators, totaling 17 indicators. Through quantitative analysis, the importance of application gaps were laws and regulations, user behavior habits, economic factors, policy and culture, and environment and technology.
Experts generally believe that laws and regulations are the most critical. At present, the Physician Law, Personal Information Protection Law and the legal provisions on the quality and data responsibility of AI auxiliary equipment are not perfect. Legal norms are the basis for defining the legality of home remote care, so they are given priority.
Followed by user behavior habits, user acceptance directly affects the implementation of telecare and AI diagnosis and treatment. Especially for the elderly over 50 years old, they need to learn how to accurately upload their health data to the application so that doctors can diagnose and track them.
Economic factors ranked third. Although the government provides certain health insurance subsidies, especially for residents in remote areas, residents in these areas may prefer community care to home remote care, because the elderly may feel lonely when they live alone, and they need interpersonal communication and social activities.
Policy and culture and environment and technology are relatively less important, mainly because these factors are greatly influenced by economic and environmental changes. Additionally, the government's policy attitude and direction may change in the future.
Discussion
Strategic analysis of laws and regulations
In the post-pandemic era, experts generally believe that the "Physician Act" will gradually be fully opened, allowing physicians and patients to legally conduct remote diagnoses and treatments without the need for face-to-face interactions. This has become an inevitable development trend. Regarding how patients can obtain medications during home remote care, practices from abroad can be referenced: Physicians prescribe medications for chronic disease patients through communication software, and patients then place orders on smart healthcare platforms, with the medications delivered directly to their doorstep. This method is both convenient and reduces unnecessary interpersonal contact.
During the telemedicine process, physicians can decide whether to use AI-assisted tools as needed. If any issues arise in home remote care, responsibility should be clearly defined: The decision-maker, usually the physician, should be accountable for the consequences of their decisions. However, experts also point out that when problems with AI-assisted tools themselves occur, the responsibility should fall on the device manufacturers, as this pertains to hardware issues; if errors in data lead to incorrect medical judgments, the data providers should be held accountable to address losses caused by software issues.
These discussions not only highlight the complexities faced by telemedicine in terms of legal, technical and responsibility divisions but also emphasize the importance of future medical regulations, technical standards, and responsibility delineation. Ensuring the safety and effectiveness of home remote care requires systematic and detailed consideration of these critical factors.
Strategic analysis of economic factors
Although the high cost of smart healthcare devices and 5G service fees cause many residents in remote areas to be hesitant about adopting home remote care, this care model can significantly reduce commuting and hospitalization costs. It is particularly beneficial for continuous monitoring of patients' health at home, thereby preventing higher treatment costs due to worsening conditions.
To address the economic gaps, this study proposes the following strategies:
• Utilize information technology to establish an image exchange center to reduce unnecessary tests and examinations, thereby further lowering medical costs.
• Combine big data analysis with targeted sampling reviews to curb redundant tests in the short term, including across different medical institutions.
• Review the payment standards for tests and examinations item by item to prevent excessive fees.
• Study the introduction of a partial co-payment mechanism for tests and examinations to alleviate the public's financial burden.
• To encourage large hospitals to transfer stable patients to other medical institutions, propose the following measures:
Compile rosters of medical institutions and departments in different regions of each county and city for reference by large hospitals when preparing patients for discharge.
Research incentive measures for large hospitals to refer patients.
• Strive to maintain consistency in the competitive environment of regional hospitals.
Additionally, for remote areas, the government should collaborate with base station operators and medical institutions to provide greater subsidies, ensuring that residents in these areas can benefit from home remote care. This policy should be distinct from those in metropolitan areas to ensure fair distribution and effective use of resources. Such measures not only enhance the feasibility of home remote care but also improve the overall quality and efficiency of medical services in remote areas.
Strategic analysis of policy and culture
Experts generally do not recommend fully integrating home remote care into the health insurance coverage, primarily due to concerns that this may lead to service abuse, which could be detrimental to the healthy development of telemedicine services.
Culturally, it is advised to avoid leaving elderly or chronic disease patients living alone whenever possible. Additionally, it is essential to educate individuals under the age of 30 to enable them to guide the elderly in correctly using remote care applications (Apps) and accurately uploading their health data. If an incorrect data upload leads to a misjudgment by the physician, the responsibility should be borne by the user. Such measures not only help improve the effectiveness of remote medical services but also enhance the users' sense of responsibility towards the service.
The implementation of these strategies aims to enhance the quality and safety of remote care services while ensuring cultural adaptability and clear responsibility. This ensures that remote medical services improve convenience while maintaining their rigor and effectiveness.
Strategic analysis of users' behavior habits
Firstly, strengthening information security is crucial. This includes implementing system firewalls, password protection, user authentication and installing antivirus software and antihacker tools. Secondly, it is necessary to formulate or revise cybersecurity and medical service regulations related to telemedicine and provide the necessary education and training to users [18] to mitigate potential legal, ethical, and insurance issues.
Regarding public medical habits, the adoption of telemedicine technologies and solutions should be based on the suitability of the users and the mobility of the elderly. Young people with digital literacy should be encouraged to teach the elderly how to operate and learn skills such as online consultations. As this method involves establishing a new type of doctorpatient relationship, healthcare professionals will need to learn how to use and adapt to these new technologies to care for the elderly and chronic disease patients.
Moreover, addressing user concerns about personal information leakage can enhance trust through stronger user participation mechanisms. Additionally, users should be informed about the advantages of combining AI with home remote care. For example, smart healthcare systems can automate information management, ensuring that each patient receives appropriate attention and treatment, such as regular monitoring and automatic adjustment of medication dosages. This not only improves healthcare quality and patient safety but also allows healthcare professionals to focus more on patient care rather than paperwork, reflecting the true value of smart healthcare.
The government has a responsibility to establish a secure review and monitoring system to protect the collective interests of the public and prevent the leakage of personal data. The continuity, comprehensiveness, interactivity, and timeliness of chronic disease remote care [18] make it an ideal choice, as chronic disease care requires continuous attention, and patients need to self-manage most of the time. Therefore, choosing home remote care not only meets patient needs but also effectively addresses the challenges of modern healthcare.
Strategic analysis of environment and technology
This study identifies and analyzes the four major challenges facing smart healthcare and their corresponding solutions. Firstly, regarding the issue of "who should access health data and who needs to verify the data," it is recommended that top medical teams and university medical faculty jointly take responsibility. Experts suggest lowering the cost of data acquisition and rigorously selecting high-quality data for research and patient treatment purposes.
The second challenge is the "high specialization in healthcare and information, leading to information asymmetry and a lack of a common language for deep communication." To address this issue, it is essential to enhance communication between medical personnel and technical staff to eliminate information asymmetry. The government should implement subsidy measures to encourage collaboration between the industry, technical personnel, and doctors, thereby creating and meeting market demand and ensuring the quality and efficiency of medical services.
The third challenge is the "lack of reliable medical teams." In Taiwan, this phenomenon is relatively rare, as the public can freely choose trusted medical teams, such as those from Veterans General Hospital or National Taiwan University Hospital. This choice should be elevated to a social communication level to enhance public trust in medical teams.
The final challenge is the "lack of a sustainable business model for smart healthcare." Experts propose shifting from the traditional monthly fee model to a "smart hospital" service model, which continuously provides services to the public while achieving sustained profitability. This transition not only ensures the continuous provision of high-quality medical services but also guarantees the economic feasibility and long-term development of smart healthcare systems.
These strategies aim to address the main challenges in implementing smart healthcare, promoting its development towards greater efficiency and reliability through innovation and adjustment.
Conclusion
This study mainly focuses on the market in Taiwan and discusses the strategic gap in the application of smart medical care in home remote care. Future research can be extended to other regional markets to analyze the status quo and strategy differences of home remote care in different countries to obtain more comprehensive research results. In addition, the research field should not be limited to home remote care and community care is also worthy of consideration.
At the same time, the study can further explore how smart medicine can innovate traditional medical practice and its farreaching impact on human welfare. This will not only help to deepen the understanding of the potential of smart medical care, but also promote technological innovation and application promotion in this field, thus better serving the development of global health.
Author Contributions
Conceptualization, Yunqi Yang. and Grace.T.R Lin.; methodology, Yunqi Yang.; software, Yunqi Yang.; validation, Yunqi Yang and Grace.T.R Lin..; formal analysis, Yunqi Yang.; investigation, Yunqi Yang.; resources, Yunqi Yang.; data curation, Yunqi Yang.; writing—original draft preparation, Yunqi Yang.; writing—review and editing, Grace.T.R Lin.; visualization, Yunqi Yang.; supervision, Grace.T.R Lin.; project administration, Grace.T.R Lin.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable for studies not involving humans or animals.
Informed Consent Statement
Not applicable.
Data Availability Statement
The author is willing to share all the data of the article publicly. If you need to obtain the data, please send an email to Yunqi Yang at yangyunqi0077@gmail.com.
Acknowledgments
Thanks to the professors of the National Yang Ming Chiao Tuing University, Institute of Biomedical Engineering, Taiwan and professionals from other schools for their support in expert interviews for this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ge J (2019) 5G empowers smart healthcare. China Information Community: 51-53.
- Sheng Y, Peng H, Feng Y (2019) Smart medical application based on 5G mobile network. Post and Telecommunications Design Technology: 1-5.
- Lv L, ZhangS, Dai P (2018) Exploring the interaction and conflict among stakeholders in telecare services. Journal of Medical Information 27: 49-62.
- Li JG, Tang XY (2013) Characteristics and development trend of smart medical application technology. Journal of Medical Informatics 34: 2-17
- Li J (2018) The development of smart healthcare in china against the background of digital divide. E-Government: 89-96.
- Yeoh SY, Chin PN (2022) Exploring home health-care robots adoption in Malaysia: Extending the UTAUT model. IJPHM 16: 392-411.
- Shi PY, Ku CY, Bai MC (2017) Circumstances of dementia families' use of long-term care services and reasons for non-use. Taiwan J Public Health 36: 375-85.
- Li MX, Gao XZ, Xiao BY (2010) An investigation of the current status and barriers to the development of telecare: The case of the farglory II residence. Lingdong Journal: 219-43.
- Jin XT, Dai MH (2012) A study of the economic and social impacts of population aging in Taiwan. Journal of Population: 72-80.
- Cai YZ (2011) The impact of telecare services on healthcare costs: A case study of system construction in Nantou. Taiwan: Nankai University of Science and Technology.
- Wu C, Lin Y, Sun Z (2013) Zero distance care for the elderly: Development and application of community home distance care. Taiwan Gerontology Forum: 1-13.
- Luo YW (2019) A study of one-to-one service marketing strategy for smart healthcare: A case study of company a's service to hospital f. Taiwan: National Central University.
- Yuan F (2002) Social research methods. Taibei: Wunan
- Posen (2013) Teaching and research methods: Interview.
- Deng Z, Zeng G (1989) The connotation and Application of Hierarchical Analysis (AHP). Chinese Journal of Statistics 27: 13707-13724.
- Chen YJ, Chen YF, Li MX (2009) Establishing a multi-architecture performance evaluation model with analytic hierarchy process method and hierarchical consistency analysis 9. Sunrise Business Review 8: 49-65.
- Chu Z (2009) Analytic Hierarchy Process (AHP) theory and practical.
- Xu Z, Tang Y (2008) Current situation and future of remote home care. Taiwan Journal of Gerontology and Gerontology 3: 272-85.

Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences