Abstract
Variability in the organisation and management of hospital care for COPD exacerbations
Intense intensifications of persistent obstructive pulmonarydisease (COPD) represent over 10% of the totalacute clinical affirmations in the UK, 1 and for 5.6% of all maleand 3.9% of all female deaths. 2 Many passings happen during, or shortly after, emergency clinic admission. An review of care in 46 UK medical clinics in 1997 showed widevariation in cycle of care and results that couldn't be accounted for by case-mix.3,4 Since then public guidelines and norms for the administration of intense confirmations with COPD, 5–7 have been distributed that incorporate definitive recommendations for the interaction of clinical consideration and have provided instances of good hierarchical practice that areevidenced based. A resulting 30 emergency clinics review of acute hospital care of COPD8 again noticed that in spite of the publication of rules there stayed set apart betweenclinic fluctuation. An extra and new finding was thatprocess of care and result showed up more regrettable in smaller hospitals with least asset proposing a connection between these factors. The a lot bigger investigation introduced here gathered information in 2003–2004 about the assets, association and clinicalcare accommodated intense intensifications of COPD in hospital. Detailed data on assets accessible to individual units, association of care inside units, and cycle of carefor the individual patients is depicted and analyzed with published public recommendations. A past distribution from the review information introduced heredescribes the review procedure exhaustively, and has high-lit the connection between tolerant results (mortal-ity, length of stay and re-affirmations) and parts of the carein taking part units. 9 In contrast, this paper centers around the assets available to, and the association of care gave by, individual unitsin examination with acknowledged public direction. Interaction ofcare offered to singular patients remembered for the review isalso considered according to best practice. The largeamount of information given by units across the UK gives aunique unmistakable outline of the route patients with COPD exacerbations are overseen when conceded to hospital. Previous distributed reviews have proposed inadequateprovision and use of assets for units to effectively and securely deal with all patients with COPD exacerbations. Despite clear public guidance 5–7 it was indistinct whether UK medical clinics had the option to draw in adequate assets tocomply with public proposals, and to diminish the variability in assets accessible and association of care between units.
Author(s):
Vsevolod Telezhkin
Abstract | PDF
Share this

Google scholar citation report
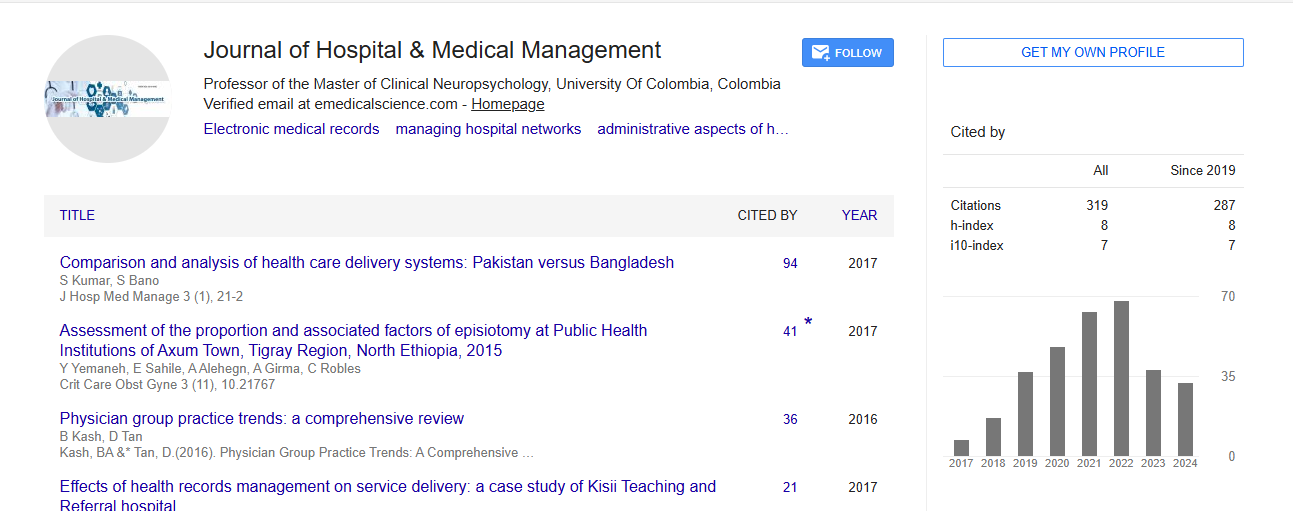
Citations : 319
Journal of Hospital & Medical Management received 319 citations as per google scholar report
Journal of Hospital & Medical Management peer review process verified at publons
Abstracted/Indexed in
- Google Scholar
- China National Knowledge Infrastructure (CNKI)
- WorldCat
- Publons
- International Committee of Medical Journal Editors (ICMJE)


Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences